The July 16, 2015 Local Coverage Determination (LCD) Lower Limb Prostheses policy that was proposed would have reverted patient care to a 1970’s standard. O&P organizations and patients joined to object to the policy, in the form of a White House petition, comments submitted to CMS, testimony at the hearing, letters from researchers whose work was cited, a rally in front of the HHS headquarters, meetings with CMS, etc. (Read all the actions taken.)
The policy was not enacted but it has not been removed from the website of CMS and its contractors, so O&P advocates have continued to voice their objections. On April 28, after efforts from the American Orthotic & Prosthetic Association, the House Oversight and Government Reform Committee released a letter to HHS Secretary Sylvia Mathews Burwell, criticizing the prosthetic LCD efforts of CMS and its contractors, and launching an oversight inquiry with a request for a substantial collection of documents. We will post updates of progress.
On April 26-27, O&P professionals, students, and patients visited Capitol Hill to meet with legislators to advocate for fair treatment of O&P providers and patients. One clinician met with Senate Majority Leader, Mitch McConnell (R-KY), who then authorized a letter to CMS Acting Administrator, Andy Slavitt regarding the 2015 LCD Policy, its status, and the workgroup that has been assembled to evaluate CMS’ O&P policy. Read the letter from Sen. McConnell to Andy Slavitt. AOPA will post any further correspondence.
Adrianne Haslet-Davis, who lost her leg as a spectator during the Boston marathon bombing in 2013, is returning as a participant. She’s running on behalf of the nonprofit Limbs for Life, raising money — over $14,000 so far — to provide prosthetic limbs for those that need but can’t afford them.
In 2015, Adrianne, a professional ballroom dancer, danced across the finish line.
In 2014, she walked across the finish line with her 2 brothers who ran the marathon.
Adrianne Haslet-Davis, Boston Marathon bombing survivor and amputee, throws out the first pitch before the Blue Jays play the Red Sox at Fenway Park on April 15, 2016. April 15 is “One Boston Day”, to celebrate the resiliency, generosity, and strength demonstrated by the people of Boston and those around the world in response to the tragedy of April 15th, 2013.
The Centers for Medicare & Medicaid Services (CMS) issued a final rule December 29, 2015 that would require patients to obtain Prior Authorization for most lower limb prosthetics.
However, it may be a while before patients will need to obtain prior authorization before receiving prosthetic care. While the rule is in place beginning February 2016, we have some indications that: (1) CMS is more likely to take an incremental approach—regional steps with a limited number of devices seems more likely than a national rollout on all prosthetics; (2) CMS may be interested to see how the draft LCD follow-up proceeds before rolling out prosthetic Prior Authorization; (3) they pledge to take steps to avoid delay in patient access to care, and to try to minimize, if not eliminate the prospect that there are post-payment audits on medical necessity issues after a Prior Authorization has been secured, which could push the date for implementation of Prior Authorization for prosthetics 6 -12 months later.
While AOPA is still concerned that the prior authorization process will delay patient access to prosthetic devices, providers will have more time to prepare than initially expected, and should be able to comply with this new rule by the time it affects patients. Since prior authorization is premised explicitly on the need to control unnecessary or excessive utilization, clearly those classes of devices showing -40+{cd9c44e368fb6cee2d09ae9816b0d094fbe47d90389af7031507558183226368} reduction in utilization since 2010 (K3 and K4 advanced prosthetics) should not be on the list of codes subject to prior authorization.
The study that started the “Mobility Saves” movement has now been published in a peer-reviewed journal. The recent Military Medicine Supplement published the study: “Economic Value of Prosthetic Services Among Medicare Beneficiaries: A Claims-Based Retrospective Cohort Study”
Military Medicine is the official journal publication of the Association of Military Surgeons of the United States (AMSUS), and this edition arises in conjunction with the topics covered at the December annual meeting of AMSUS.
This study demonstrates, using four years of Medicare data, that timely O&P intervention saves payers’ money.  Dr. Allen Dobson, the author of this research, presented his work at the AMSUS meeting, and the attached manuscript will make this work widely available for citation for use by payers (including both Medicare and private sector providers), and others to show the value of O&P care (page 18).
This edition also includes the manuscript developed by a Multi-Disciplinary Task Force headed by John Fisk, M.D., with physician representatives from both physical medicine and rehabilitation, and orthopedic surgery, a physical therapist, and certified O&P professionals around key issues on the orthotic treatment team, distinctions between off the shelf (OTS) and customized orthotics, the importance of the orthotist’s notes and records, and other key clinical issues (page 11). This publication is particularly timely in establishing this valuable consensus viewpoint at a time when orthotic care, and its reimbursement are attracting greater attention and scrutiny.
There are also several reasons why we are especially pleased to see both of these articles appearing in Military Medicine. This journal is a peer-reviewed medical journal, listed in the Index Medicus, which conveys substantial credibility for these papers, placing it in the top tier for purposes of medical citations, and because of the importance of topics covered in this journal to Congressional Appropriations and Department of Defense matters, Military Medicine is circulated to all Congressional Offices, giving these messages great reach to our lawmakers.
An exoskeleton prototype used for neuro-motor rehabilitation. IMAGE: BSIP/UIG VIA GETTY IMAGES
BY ARIEL BOGLE
Australian scientists hope a device about the size of a matchstick will one day help people with spinal cord injuries get back on their feet.The device, a stent-electrode recording array or stentrode, could allow patients to control powered body armour, known as exoskeletons, or bionic limbs using only their thoughts, researchers announced Tuesday at the University of Melbourne.The stentrode will be implanted in a blood vessel that sits over the brain, and will turn brain signals into electrical commands that could wirelessly move the exterior mechanical technology. Currently, most exoskeletons are controlled by a joystick that is operated manually.
A collaboration between the Royal Melbourne Hospital, the Florey Institute of Neuroscience and Mental Health and the University of Melbourne, the findings were published Tuesday in the journal, Nature Biotechnology.
The stentrode device went through hundreds of design changes before researchers were satisfied it met their requirements of being light, flexible, bio-compatible and small enough to be threaded into a one millimetre blood vessel.
IMAGE: UNIVERSITY OF MELBOURNE
Speaking at a press conference Tuesday, Thomas Oxley, a neurologist at the Royal Melbourne Hospital, said the project began when he had the idea that thought control of bionic limbs could be achieved without implanting a device through open brain surgery.
Preclinical studies have shown that by putting the stentrode in a blood vessel near the motor cortex, a key control centre for the brain, you can get the same recording as people previously obtained by surgically inserting something directly into the brain. He proposed that, using the stentrode, patients will one day be able to control mechanical limbs with their thoughts.
“The idea is the device is much less invasive than previous attempts at doing this and can be implanted longterm,” said Terry O’Brien, head of medicine at the Departments of Medicine and Neurology, the Royal Melbourne Hospital and University of Melbourne. “There is no clinical device that does this at the moment.”
The stentrode can record brain signals from within a blood vessel next to the brain. These thoughts are captured, decoded and passed wirelessly through the skin to enable control of an exoskeleton.
It could also have applications far beyond assisting those with paralysis, he added. The stentrode could be used to record brain waves for those with conditions such as epilepsy, helping to predict when they are about to have an attack. “The applications are incredibly broad, and that’s what makes it so exciting,” O’Brien said.
The device, which has so far been tested on sheep, will undergo its first human trials in 2017. According to a statement from the University of Melbourne, patients will have to, in many ways, learn to walk and stand again by getting familiar with “coding” the signals to their exoskeleton. “With our device, you’ve essentially connected an electronic limb to the patient’s brain, but they have to learn how to use it,” Oxley said, according to the statement.
Nick Opie, a biomedical engineer at the University of Melbourne, told reporters the team hoped the cost of the device, after it has undergone human testing and is ready for market, would be similar to the cochlear implant — around A$15,000 (US$10,567) to A$20,000 (US$14,089). They predict it will be ready by 2022.
It is also hoped the stentrode will be as important to medicine as the cochlear implant, which was invented in Australia. “What cochlear implants have done for hearing, we want to do for mobility,” Opie said.
Interest in bionic limb and exoskeleton technology has been developing rapidly in recent years. Earlier in February, SuitX announced a new Phoenix exoskeleton that aims to replicate human gait.
On December 29th, the Centers for Medicare and Medicaid Services (CMS) released the long anticipated final rule regarding Medicare prior authorization of certain DMEPOS, including most lower limb prostheses. The final rule, which will be published in the December 30, 2015 Federal Register, will be implemented 60 days after it publication. AOPA has reviewed the final rule, and offers the following preliminary thoughts and comments regarding the provisions of the final rule. AOPA’s primary concern with prior authorization of prostheses is, and always has been, that it will critically delay timely access to the provision of prosthetic devices that are crucial to the rehabilitation needs of Medicare beneficiaries. In the final rule, CMS acknowledged that proper access to medically necessary care is of the utmost importance, but indicated that it will use sub-regulatory processes to determine appropriate timelines for making prior authorization decisions. These sub-regulatory processes are inherently arbitrary in that they do not allow for public input and or comment regarding their appropriateness. AOPA remains concerned that prior authorization of any kind will only serve to hinder the delivery of medically necessary prosthetic care within reasonable timeframes. Another concern that AOPA expressed in its comments on the proposed rule that was not sufficiently addressed in the final rule is that prior authorization does not equate to a guarantee of claim payment nor does it eliminate the exposure of the claim to additional audits.  While the final rule states that an affirmative prior authorization decision indicates that the required documentation for claim payment is present, it also reiterates that it is not an initial claim determination and the claim may ultimately be denied for technical reasons such as invalid proof of delivery documentation. AOPA met with representatives from the Office of Management and Budget (OMB) in August while they were reviewing the proposed rule and registered concerns about the above issues. The few seeming new wrinkles in the final rule is that implementation will not be immediate and universal, but there will be a Master List of 135 HCPCS codes eligible for inclusion in prior authorization. It appears there will a phase-in process, meaning not all 135 codes will be subject to prior authorization immediately. Rather, the final rule indicates that CMS will establish a subset of the master list that will determine which HCPCS codes require prior authorization as part of the initial implementation of the final rule. While the master list includes lower limb prosthetic HCPCS codes that meet or exceed the $1,000 threshold, it remains to be seen which codes will be included in the initial list of codes that will be subject to prior authorization. While the current list does not include any orthotic codes, AOPA remains concerned that future updates to the master list may include orthotic codes that meet the criteria for inclusion in prior authorization. At first glance, the final rule does not recognize two key facts from Medicare’s own data:
There is not a problem of unnecessary utilization of lower limb prosthetics, and the -14{cd9c44e368fb6cee2d09ae9816b0d094fbe47d90389af7031507558183226368} reduction in prosthetics payments over the 2010-13 period proves that;
Today, Medicare prosthetic patients are 35{cd9c44e368fb6cee2d09ae9816b0d094fbe47d90389af7031507558183226368} LESS LIKELY to receive an advanced tech prosthetic device than they were just 5 years ago (2005-2009).
In addition, the final rule acknowledges AOPA’s concern regarding the need for a more timely response to prior authorization requests but elects to define these timeframes through sub regulatory processes that do not allow for public comment or input. While AOPA will review the final rule more closely in the coming days, After its preliminary review,  AOPA believes that the final rule fails to address AOPA’s concerns regarding the implementation of a prior authorization program that:
Does not appear to constitute a guarantee of payment; and
Retains the payment threshold of $1,000 for inclusion in prior authorization
Does not assure that providers would not be subject to post-payment/RAC audits on the very same issue of medical necessity; and
Uses sub-regulatory processes to define appropriate timeframes for response to prior authorization requests; and
Exceeds its authority to initiate a limited pilot on prior authorization, done only in selected areas (as was done with power mobility devices) to a national policy impacting all amputee beneficiaries nationwide.
AOPA will provide additional analysis of the final rule as it becomes available.
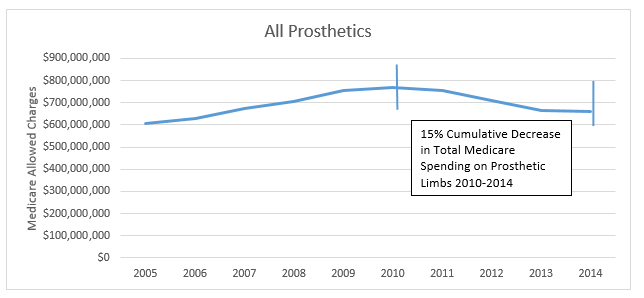
What has happened to Medicare’s Spending on Prosthetics since 2010?
AOPA has analyzed the data, and the picture is clear. Medicare spent 15{cd9c44e368fb6cee2d09ae9816b0d094fbe47d90389af7031507558183226368} less in 2014 than in 2010 on prosthetics.
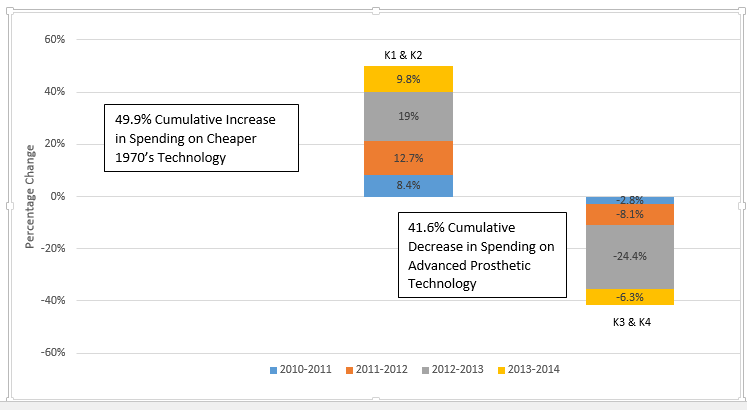
Medicare spending on advanced prosthetics has trended down 40{cd9c44e368fb6cee2d09ae9816b0d094fbe47d90389af7031507558183226368}, while spending on older technologies has trended up – 35{cd9c44e368fb6cee2d09ae9816b0d094fbe47d90389af7031507558183226368}. Overall spending has decreased by 14{cd9c44e368fb6cee2d09ae9816b0d094fbe47d90389af7031507558183226368} since 2010.
Year
All Prosthetic Spending
Year
All Prosthetic Spending
2005
$607,797,189
2010
$770,462,739
2006
$628,220,869
2011
$756,265,554
2007
$676,421,628
2012
$710,599,456
2008
$704,604,327
2013
$664,405,441
2009
$753,410,033
2014
 $662,585,471
Medicare Spending has INCREASED on antiquated prosthetics and DECREASED on Newer Technologies.
2010
2011
2012
2013
2014
Total {cd9c44e368fb6cee2d09ae9816b0d094fbe47d90389af7031507558183226368} Change  2010-2014












{kind=link}